Introduction of the payment for performance model in acute hospitals in the Republic of Serbia
Mirjana Milosevic a, Marina Topalovic a, Simo Vukovic a, Biljana Trivic Ivanovic a, Drasko Lazovic a
Introduction
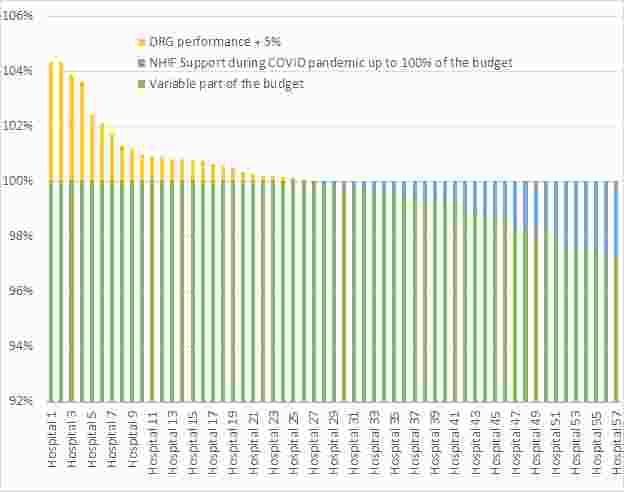
In the Republic of Serbia, the NHIF is the dominant buyer of services of publicly owned health institutions with the application of historical budgeting, which means that it concludes a contract with hospitals based on the contract from the previous year. Currently, the RHIF transfers money to hospitals in the form of line budget, which greatly limits the work of management, given that there is no shifting of money from one line to another. An additional, existing circumstance is that the budget of hospital is determined on the basis of its capacity (beds and staff). After several years of preparation and implementation, as of January 2019, the DRG payment model has been applied. A 6.0 version of the Australian classification is used, which also has accompanying software for data grouping. As implementation is gradual, currently 95% of the financial resources defined in the budget are transferred each month to health institutions by purpose, while the remaining 5% of financial resources is a variable part of the budget and its payment depends on the DRG performance (4%) and quality indicators (1%) (Graph1). All 57 public acute hospitals are funded under this model (Graph2). Implementation, analysis and further improvement are carried out within the Second Serbia Health Project of the MoH.
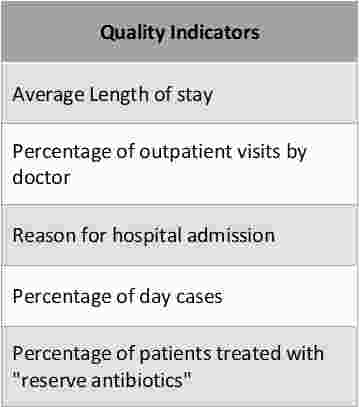
In addition to the DRG effect of hospitals, a mechanism for measuring the performance of attending physicians has been created (Graph3). The mechanism is centralized, as for the performance of hospitals, it is determined in the NHIF on the basis of data from the invoices.
Methods
Descriptive statistics, Description of data analysis results
Results
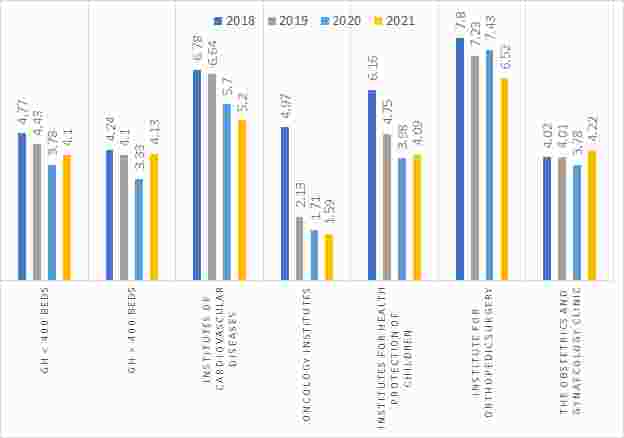
Effects of DSG payment model:- Reduction of ALOS (2018: 5.5 days, 2019: 4.8 days, 2020 before COVID : 4.2, 2021: 4.3) (Graph4)
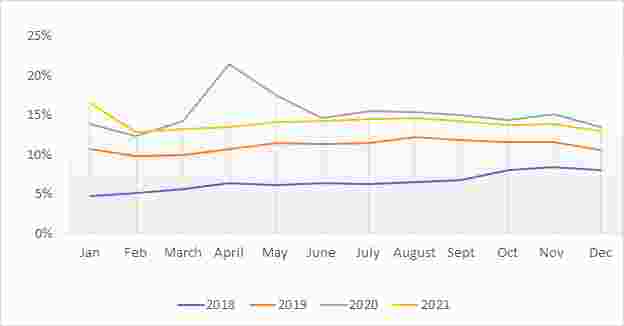
- Increasing the sameday hospital services (Graph5)
- Issuance of centers of excellence
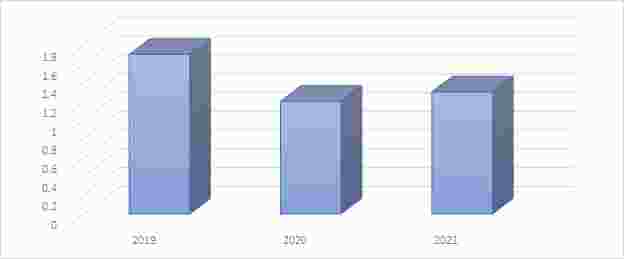
COVID pandemic has a strong impact on hospitals performance:- Decrease of the case-mix index (2019: 1.7, 2020: 1.2, 2021: 1.3) (Graph6)
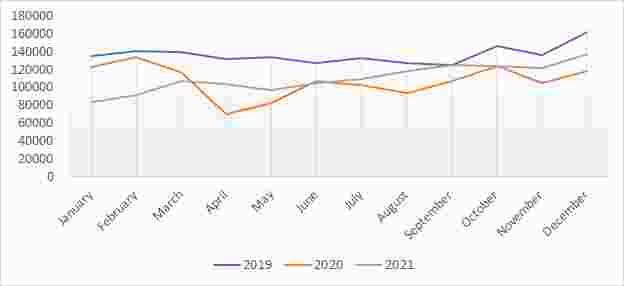
- Decrease in the number of hospitalizations (2019: 1.63M, 2020: 1.28M, 1.32M) (Graph7)
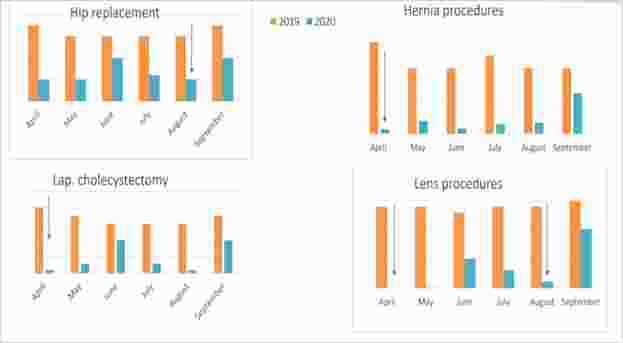
- Significant decrease in the volume of elective surgical procedures (consequently the creation of a waiting list) (Graph 8)
Conclusions
Despite the deviations caused by COVID, payment for performance model has led to positive effects on hospital operations. The next steps to improve the payment model are to increase the variable part of the budget of hospitals affected by the DRG performance, abolish the line budget and introduce a program budget based on efficiency and quality of health care (treatment outcomes).
Graph1 - Hospital Payment model
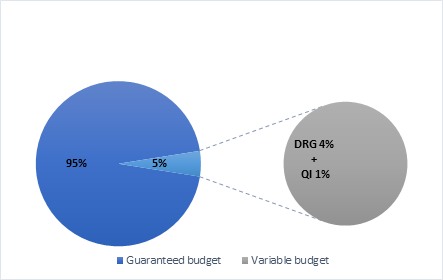
Graph2 - Hospital's budget
Graph4 - ALOS
Graph5 - The share of the same day services in total number of episode care
Graph3 - Doctor's performance measurement - criteria

Graph6 - Case-mix index
Graph7 - Number of episodes of care (DRGs)
Graph8 - Elective surgeries
a Second Serbia Health Project Ministry of Health of the Republic of Serbia, Serbia
Original Version in PDF